Managing neurodivergent capacity
I’m a late-diagnosed autistic. This means I spent most of my life trying to function according to instructions written for a nervous system that is not my own. Like a lot of neurodivergents, I learned to override instead of regulate. We mask, we suck it up and push through. Until we can’t anymore. We recover just enough to do it again while the time between shutdowns gets shorter and shorter. At some point we experience a systemwide shutdown we don’t even know to recognize as autistic burnout.
Late-diagnosed or not, none of us get a user manual for our neurology. We inherit the neurotypical way of life and assume any damage comes from personal weakness instead of a nervous system mismatch. We start to believe we are failing at things other people handle naturally. So we compensate harder. A lot of us reach a point in our lives where nothing works at all anymore.
I’ve been through all of this. I found my own way out through a lot of trial and error, without understanding what I was doing or why some things worked. It wasn’t until I recognized the same patterns in my son and applied the same strategies that I realized there is an actual structure behind it. Systems that govern capacity, shutdown, burnout and recovery. Systems that can be described, monitored, and regulated.
The Reservoir
Every autistic person has a finite amount of capacity their nervous system holds at any given time. Think of it as a reservoir. It overlaps conceptually with what stress researchers call allostatic load: the cumulative physiological cost of chronic nervous system strain. Every waking moment, stress situation, social demand, sensory input, and every moment of masking drains it. As long as the reservoir stays above a certain threshold, you appear fine. You might even feel fine. But before you do finally shut down, you can usually feel it approaching. What you where feeling is the reservoir draining.
But this is where most people get it wrong. This is where I got it wrong myself.
Everything that went wrong was happening in the first half of the reservoir. We drain in real time but don’t respond until the symptoms are serious enough to demand our attention. By the time they appear, the reservoir is already critically low. We are not catching the problem. What we are seeing is the consequence of a problem that started long before we responded.
The biggest mistake we constantly make: as soon as symptoms disappear, the instinct is to go back to the conditions that caused them. But the reservoir has only climbed back above the threshold where symptoms are visible. We return at 40 or 50 percent. Then the cycle repeats. Each time with less capacity. Each time with faster collapse. And each time, the ability to even sense the onset of collapse grows more and more numb.
This is exactly the pattern that leads to autistic burnout. And if recovery stays insufficient long enough, the symptoms escalate into territory that many clinicians misdiagnose as psychiatric disorder. In some cases people go like this for years. They go from doctor to doctor, each with their own bespoke diagnosis for what’s wrong with them according to the DSM-5. This has been documented extensively. It happened in my own family.
The pressure to function like a neurotypical person is high, especially if you were diagnosed late. But you need to understand: your nervous system is carrying far more load than the people around you realize, and probably more than you realize yourself. A neurotypical brain filters enormous amounts of sensory, emotional, and environmental information automatically. The neurodivergent brain doesn’t. We get used to carrying enormous levels of tension, pain, noise, and overstimulation. Then we mistake the absence of visible symptoms for recovery when it’s not. It is often just numbness. It is survival mode. If you are neurodivergent, you need more recovery time than you have been taught to allow yourself. Not because you are weak, but because your nervous system is doing significantly more work than you can consciously feel in the moment.
If the reservoir is your total capacity, the corridor is the environment where that capacity is maintained.
The Corridor
Within these lines is our safe space. The conditions under which we feel most capable. In Polyvagal Theory this is known as the window of tolerance. A range of sensory and emotional stimulation within which the nervous system can stay regulated. Within that corridor, the reservoir can fill overnight. We sleep, recover, and wake up with capacity.
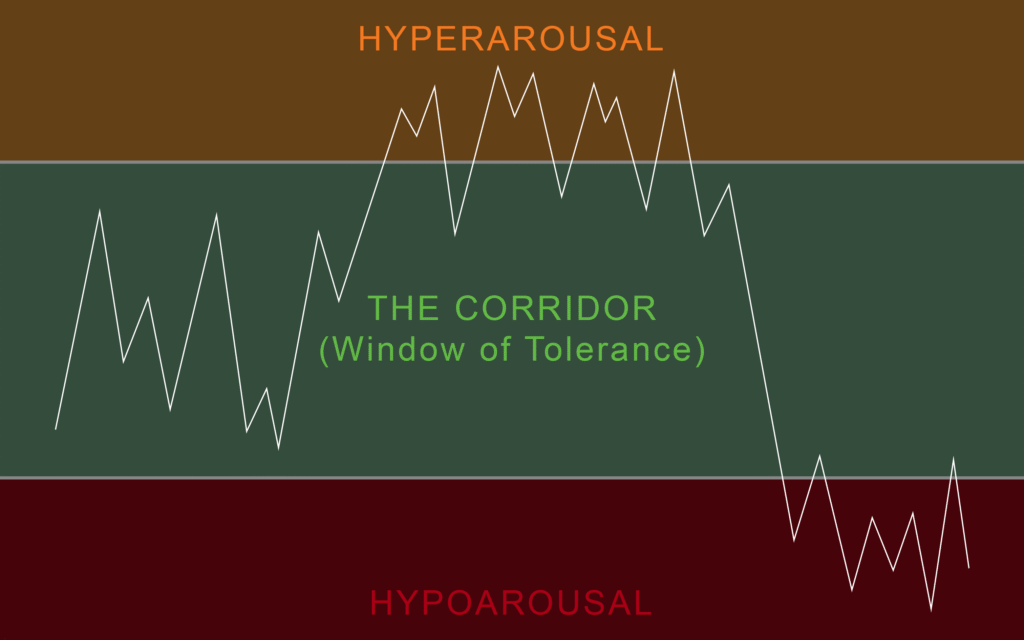
Above the corridor is where our senses get overwhelmed. It is called hyperarousal. Chronic nervous system over-activation. A fight-or-flight response that can stay on without present triggers. It shows up as intense anxiety, insomnia, hypervigilance, irritability, and startle responses. If you are subjected to sustained or extreme levels of hyperarousal, the nervous system can activate past the point where sleep alone can repair it.
If you are a high-masking neurodivergent, you are already sitting at the top of the corridor when you walk into any social environment. Masking alone is a high arousal state. This is why a single work meeting, a family dinner, or an errand-heavy Saturday can push you into hyperarousal before anything has gone obviously wrong.
When hyperarousal continues without sufficient recovery, the nervous system drops. Not back into the corridor. Below it, into hypoarousal.
If you have ever described yourself as “fine but empty,” or noticed that you stop caring about things that normally matter to you, or realized you’ve been sitting in one place for an hour without moving, you’ve probably been here.
This is the most dangerous state, because for many neurodivergent people, you start to slip into a realm that is harder to feel. Many neurodivergent individuals already have muted interoception. This is our “eighth sense.” The internal sense that tells us if we are hungry, thirsty, need the bathroom, or are in pain. A neurodivergent in hyperarousal can just feel exhausted, others can dissociate. You can get quiet, compliant, feel flat and still. Everyone around you thinks you’re relaxed. And the most insidious part is that people close to you might even prefer you this way. Even darker than that, some of us get used to this being a daily ritual. We don’t regulate and we don’t stop until we get here. In reality, your nervous system has shut down to conserve what little is left. It is collapse with a mask on. The more it happens, the closer you get to a state that can take weeks, months, or years to recover from.
Reading Your Own Signs
The journey down the reservoir is marked with signs. Everyone has them. There are thin and thick markers. Thin markers are behaviors and patterns triggered by hyper and hypoarousal events. Thick markers are physiological patterns triggered by how far the reservoir has drained. The goal is to recognize your thin markers and respond to them before the thick ones manifest.
Thin markers vary from person to person but common ones include increased anxiety, increased masking (performing harder at things that used to be automatic), anxious loops in your thinking, restlessness, loss of appetite, difficulty making simple decisions, irritability that doesn’t match the situation, and a sudden need to control your environment.
Thick markers tend to be more physiological: skin flare-ups, digestive disruption, disrupted sleep, startle responses to ordinary sounds, loss of interest in food or hobbies, difficulty speaking or finding words, skill regression, and emotional volatility that feels disproportionate to triggers.
If you are seeing thick markers in yourself, either you experienced an extreme hyperarousal event, or the drain started long before you noticed. In both cases you are operating with a narrower corridor and less capacity to absorb what comes next.
Most ND adults have never mapped their markers. Start paying attention after demanding events. How you feel during and after work, a social gathering, travel, or conflict to name a few. Write down what happens inside of you. Not just what you feel emotionally. What your body does, what your behavior does, what your routines do. Over a few weeks a pattern will appear. That pattern is your early warning system.
How the Reservoir and Corridor Affect Each Other
The more intense a hyperarousal event is, the more it drains the reservoir. The lower the reservoir drains, the narrower the window of tolerance becomes. You become less resilient and have more difficulty regulating things you could normally handle well. This in turn accelerates reservoir drain exponentially. This is why protecting the reservoir matters more than managing crises. A single bad night of sleep often exhausts more than half the reservoir.
This is also why “pushing through” feels productive in the moment and catastrophic by Friday. You are borrowing against a reservoir that compounds its losses.
Cooldowns
Once you are outside the corridor, you can only return with deliberate intervention or a lot of time spent within it. I call these cooldowns. The best ones are the ones you already know work for you. All of them benefit from reducing sensory input first (low light, low noise, fewer decisions).
Some frameworks that work across a lot of ND nervous systems:
Deep pressure. Weighted blankets, compression clothing, lying under heavy cushions, firm self-massage. Deep pressure activates the parasympathetic nervous system directly.
Rhythmic stimulation. Rocking, walking at a steady pace, drumming, music with a strong down-tempo beat. Rhythm is one of the fastest regulators because the nervous system entrains to external patterns.
Water. Long showers, baths, swimming. Particularly heavy water pressure on the back and shoulders. Water combines deep pressure, temperature regulation, and white noise in one input.
Sustained physical contact. If you have a partner or close person who understands, lying against them with steady pressure on your back or chest. Classical music or silence. No talking.
Alternating sensation. Squeeze your limbs, apply cold then warm, alternate pressure on hands and feet. This works because it forces the nervous system to process grounding input instead of looping on internal signals.
Sleep. This is most important and what so many neurodivergent people get wrong. Sleep is one of the most critical processes for nervous system repair. If you’re not getting enough, disaster is already on a timer. If your nervous system is overloaded, you might need more. If you find yourself in hypoarousal, sleep can help. If you find yourself entering hypoarousal at the same time every day, set your bedtime an hour before it comes. Never let your nervous system get there in the first place.
A possible sign during effective cooldown is the physiological sigh. A deep, involuntary double-inhale followed by a long exhale. The kind of breath you take after intense crying. This is your parasympathetic nervous system activating. The body shifting from fight-or-flight into rest-and-digest. When you feel this happening, your system is coming back down. Don’t stop yet. Stay with it.
The “Other” Nervous System
Chronic stress affects sleep quality, digestion, appetite, inflammation, muscle tension, and stress hormone regulation. But one of the most profound realizations for me was the moment I learned about the intersection between the nervous system and the gut. Not metaphorically, but mechanically. When we think neurodivergent, we think brains processing the world differently. But neurology is not contained in the brain alone. The gut contains its own massive neural network called the Enteric Nervous System, sometimes called the “second brain.”
What does that mean for us?
90% of the body’s serotonin is produced in the gut. The gut microbiome also interacts with dopamine pathways, cortisol regulation, immune signaling, and the vagus nerve. Magnesium is heavily involved in nervous system regulation and stress response. Prolonged stress can deplete it faster than the body replenishes it. Sleep disruption compounds all of this further.
Research increasingly shows higher rates of certain deficiencies and altered gut microbiome patterns in autistic and ADHD populations, particularly involving iron, magnesium, zinc, vitamin D, omega-3 fatty acids, and gastrointestinal regulation.
This does not mean every ND individual has the same deficiencies or should take the same supplements. I am not a doctor, and none of this should replace proper medical advice. But I do think many neurodivergent people spend years trying to regulate a nervous system while ignoring the biological systems that support it underneath.
My son struggled with sleep regression, regulation, and behavioral problems for months. After his doctor prescribed a supplementation plan, everything changed in just a few days. For us, understanding the principles outlined in this essay was only half the battle. Because an overloaded nervous system becomes harder to regulate when the body supporting it is also running on empty.
The Part Nobody Tells You
Many of us have been in shutdown for so long that we don’t even remember how baseline felt. We literally don’t know who we used to be when we were last okay. Just okay. Not great, not even happy. Just okay. I feel that. It used to be me. You’re going to have to start by owning your neurology first. Nobody is going to do that for you. You can’t expect anyone to respect your neurology any more than you do. And I can tell you from experience, nobody is going to give you permission to make space for it. And nobody is coming to save you. And it has nothing to do with how cruel the world is. It is a matter of neurological sovereignty.
This will be the most important skill you will ever master in your neurodivergent life. It will affect how you can show up for yourself and for others. But it is one for which you will not get any medals. Nobody is going to cheer you on, and nobody is going to pat you on the back. It’s a win between you and you. But one that everyone in your life will benefit from.
You will not do any of this perfectly at first. You will miss your thin markers. You will push through days you should have pulled back from. You will confuse hypoarousal with finally feeling calm.
The point is not perfection. The point is that the reservoir is real, the corridor is real, and your signs are consistent even when your awareness of them isn’t. Once you see the pattern, you can’t unsee it. And every time you catch a thin marker and respond to it instead of overriding it, you are building a different relationship with your own nervous system.
One where you stop asking “why did I collapse” and start asking “where was I when the drain began.”